Transduction-Transplantation Mouse Model of Myeloproliferative Neoplasm
Introduction
Transduction-transplantation is a useful method to model hematologic malignancies in mice. This technique has been particularly valuable for studying myeloid malignancies dating back to the first demonstration that ectopic expression of BCR-ABL1 could faithfully recapitulate chronic myelogenous leukemia in mice. This technique has subsequently facilitated the extensive study of JAK2 and MPL mutated myeloproliferative neoplasm (MPN).
MPN are a group of hematologic malignancies characterized by the overproduction of mature myeloid cells and bone marrow fibrosis. These diseases generally arise from the clonal expansion of a hematopoietic stem cell that has acquired a somatic mutation in either Jak2, MPL, or CALR. Transduction-transplantation JAK2 and MPL models exhibit the clinical features of polycythemia vera and myelofibrosis-. Recently, a mouse model of calreticulin-mutated MPN has also been generated with the transduction-transplantation method. These mice develop an essential thrombocythemia-like disease with increased platelets, increased number of megakaryocytes, and bone marrow fibrosis. Together, these models have not only provided the opportunity to gain insight into the molecular pathogenesis of MPN, but also the capacity to develop and study therapeutics in a pre-clinical setting.
This manuscript provides a detailed description of transduction-transplantation methodology with a focus on the CALRdel52 mutation. This technique involves transplantation of retrovirally transduced bone marrow cells expressing the mutant construct into irradiated syngeneic recipient mice.
Protocol
This study was approved and carried out in accordance with the recommendations by the Institutional Animal Care and Use Committee at University of California, Irvine. All procedures were performed under isoflurane anesthesia and all efforts were made to minimize suffering.
1. Generation of Ecotropic Retrovirus
Prepare high-quality plasmids with a concentration of at least 1 µg/µl using either a commercial maxi-prep kit or cesium chloride purification. NOTE: These include an MSCV backbone vector encoding the gene of interest (in this case CALR) and marker of choice (GFP, Neo, etc.) as well as an ecotropic packaging plasmid, encoding gag-pol-env (referred here as plasmid).
Thaw and expand low-passage 293T cells in DMEM supplemented with 10% FBS and L-glutamine with penicillin/streptomycin (D10). Plate 5 x 10 cells in a 10 cm tissue culture-treated dish in a humidified tissue culture incubator at 37 °C and 5% CO2.
Expand 293T cells in culture. On the day before transfection, wash cells by adding 1 ml PBS and aspirate supernatant into a vacuum flask.
To trypsinize cells, add 2 ml 0.05% trypsin and incubate dishes in a humidified tissue culture incubator for 2 - 3 min at 37 °C and 5% CO2.
To stop trypsinization, add 3 ml D10 to dish and transfer cells to a 15 ml conical tube. Spin cells at 400 x g for 10 min.
Aspirate supernatant into a vacuum flask and resuspend cell pellet in 2 ml D10.
Count the cells by trypan blue exclusion using a hemocytometer.
Seed 2 x 10 cells per dish into three 10 cm tissue culture-treated dishes per virus generated. NOTE: For optimal results, do not allow the cells to exceed 30 - 50% confluence at time of transfection or a poor virus yield may be obtained.
Immediately before transfection, aspirate media into a vacuum flask and replace with 5 ml fresh D10.
For every 10 cm Petri dish to be transfected prepare an individual sterile 1.5 ml microcentrifuge tube.
Pipette 760 µl of reduced serum media into each microcentrifuge tube, then carefully add 40 µl of transfection reagent directly into the media. Incubate tubes in the tissue culture hood at room temperature for 5 min.
Add 30 µg of MSCV vector with gene of interest (15 µg if using empty vector) as well as 5 µg of plasmid to each respective tube and mix gently by pipetting up and down. Incubate at room temperature in the tissue culture hood for an additional 15 min. NOTE: Smaller vectors tend to have higher viral yields.
Carefully add the total volume of each reaction (approximately 800 µl) drop-wise into its respective 10 cm Petri dish and gently tilt the dish from side to side to mix. Return cells to the humidified tissue culture incubator.
Following an 8 hr or overnight incubation in tissue culture incubator, aspirate media into a vacuum flask and gently replace with 10 ml of fresh D10.
At 48 hr post-transfection collect supernatant into a 35 ml syringe and filter through a 0.45 µm membrane to remove cell debris.
OPTIONAL: Place 10 ml fresh D10 back on the 293T cells and additional virus may be harvested at 72 hr post-transfection.
Dispose of 293T cells in biohazard waste when no additional virus is collected.
Aliquot viral supernatant into single use volumes (for example 1 ml for virus titer or 6.5 ml for BM infection). Flash-freeze virus with liquid nitrogen and store virus at -80 °C. NOTE: Avoid repeated freeze/thaw cycles as they greatly reduce virus titer.
2. Determine Relative Viral Titer by Flow Cytometry
Thaw 3T3 cells and maintain in D10. Culture the cells in a 10 cm tissue-culture treated dish in a humidified tissue culture incubator at 37 °C and 5% CO2.
Perform viral titer in triplicate. To prepare cells, wash cells by adding 1 ml PBS and aspirate supernatant into a vacuum flask.
To trypsinize cells, add 2 ml 0.05% trypsin and incubate dishes in a humidified tissue culture incubator at 37 °C and 5% CO2.
To stop trypsinization, add 3 ml D10 to dish and transfer cells to a 15 ml conical tube. Spin cells at 400 x g for 10 min.
Aspirate supernatant into a vacuum flask and resuspend cell pellet in 2 ml D10.
Count the cells by trypan blue exclusion using a hemocytometer.
Seed 3T3 cells at a density of 1 x 10 cells into fifteen 60 mm tissue culture-treated dishes and incubate overnight.
Make 1:3, 1:10, 1:30, and 1:100 dilutions of thawed viral supernatant using D10 in a total of 1 ml. Also include a virus-free control.
Aspirate media from 3T3 cells into a vacuum flask and replace with 4 ml of D10.
Overlay the 3T3 cells with the dilutions of viral supernatant and add polybrene to a final concentration of 8 µg/ml to each dish. Incubate for 48 hr in the tissue culture incubator at 37 °C and 5% CO2.
Determine relative viral titer by flow cytometry:
To wash cells, aspirate the media into a vacuum flask and add 5 ml PBS.
Aspirate the PBS into a vacuum flask. Add 1 ml 0.05% trypsin and incubate at 37 °C for 2 - 5 min to detach cells from dish.
Add 3 ml D10 and pipette up and down to detach any remaining cells from the plate. Transfer the cells to a FACS tube and centrifuge at 400 x g for 10 min.
Decant supernatant and wash cells with 3 ml PBS. Centrifuge at 400 x g for 10 min and decant supernatant. Resuspend in 200 µl PBS.
Run cells on a flow cytometer. Collect between 20,000 - 30,000 events within the live cell gate (determined by FSC vs. SSC) and calculate the percentage of GFP and GFP cells. NOTE: The viral titer is considered acceptable when the 1:30 dilution of viral supernatant yields at least 50% GFP 3T3 cells. If this dilution results in less than 50% GFP cells then suboptimal transduction results may be obtained. The calculation to determine viral titer was adapted from Limon et al., Blood (1997).
To determine relative virus titer, use the equation: virus titer = particle forming units (PFU)/ml = [(Number of 3T3 Cells × Frequency of GFP Cells) / Volume of Supernatant (ml)] × Dilution Factor.
3. Transduce Donor Bone Marrow Cells
To prepare donor mice for bone marrow (BM) harvest, first anesthetize mice by isoflurane vaporizer with a flow rate of 5% combined supplemental oxygen at 1 L/min. Pinch foot to assess responsiveness. NOTE: Donor mice (less than 8 weeks old) should be prepared 5 days prior to bone marrow harvest (8 days prior to transplantation). One donor mice will provide enough cells for at least 2 recipients.
Inject 150 mg/kg 5-fluorouracil (5-FU) via retro-orbital injection in anesthetized mice using a 27 G × ½" needle. CAUTION! 5-FU an anti-cancer chemotherapeutic agent. Always handle 5-FU inside a certified chemical fume hood or a ducted biosafety cabinet. Consult with the institution's laboratory and animal safety committee to determine appropriate labeling of mice treated with 5-FU.
Position the anesthetized mouse on its side and restrain by using both the thumb and index finger such that the eye protrudes slightly from the head.
Starting with the needle lateral to the medial canthus and with the bevel facing up, insert the needle at a 45° angle in the medial direction and stop when the needle is halfway inserted. Slowly inject cells and remove carefully remove needle. NOTE: If this technique is performed correctly, the eye should retract slightly and no resistance should be felt upon needle insertion.
Examine mouse for any signs of injury such as swelling or bleeding.
Harvest bone marrow 5 days after 5-FU treatment (3 days prior to transplantation).
Anesthetize mice by isoflurane vaporizer with a flow rate of 5% combined supplemental oxygen at 1 L/min. Pinch foot to assess responsiveness.
Sacrifice mouse by cervical dislocation. Sterilize mouse by spraying generously with 70% EtOH until fur becomes wet.
Using dissecting scissors, make an incision in the skin and dissect the fascia away from the leg muscles. Next, dissect the leg away from mouse by severing the femur at the hip and the tibia at the ankle.
Bend the leg into a "L" shape and separate each leg bone by cutting at the knee joint with dissecting scissors.
To remove cartilage at the distal ends of each leg bone, use the dissecting scissors to gently scrape muscle towards one end of the leg bone until cartilage is disengaged.
Using a syringe with a 27 G x ½ inch needle, flush each leg bone with PBS supplemented with 2% FBS over a 100 µM nylon membrane in a 50 ml conical tube. Flush bone until bone turns white to maximize the number of cells harvested.
Use the plunger of a syringe to mash cells through the nylon membrane into the 50 ml conical tube to obtain a single cell suspension. Repeat with other mouse leg.
Centrifuge cells at 4 °C for 10 min at 400 x g and discard supernatant. Resuspend BM in 5 ml ammonium chloride potassium (ACK) buffer to lyse red blood cells. Incubate cells on ice for 10 min.
Fill tube with PBS to stop cell lysis. Centrifuge cells at 4 °C for 10 min at 400 x g and discard supernatant. Repeat lysis step if the BM pellet has red color.
Resuspend in 5 ml PBS and count cells by trypan blue exclusion using a hemocytometer.
Resuspend cells at 2 x 10 cells per m with 2x pre-stim cocktail which contains DMEM supplemented with 20% FBS, L-glutamine, penicillin/streptomycin, IL-3 (14 ng/ml), IL-6 (24 ng/ml), and SCF (112 ng/ml). Plate 2 ml per well in 6 well plates.
Incubate the cells overnight at 37 °C and 5% CO2.
Add 2 ml of viral supernatant to each well containing BM cells and add polybrene (8 µg/ml). Spin plates at 30 °C for 90 min at 1,500 x g then return plate to the tissue culture incubator overnight.
Pipette cell suspension into conical tubes and centrifuge at 4 °C for 10 min at 400 x g, do not discard the plate. Resuspend cells in 2 ml fresh 2x pre-stim cocktail per well and return to the original wells.
Perform a 2 spinoculation by repeating steps 3.7-3.9.
4. Transplant Donor Cells into Recipient Mice
Prepare syngeneic recipient mice for transplant with lethal dose total body irradiation < 24 hr prior to injection of BM cells. NOTE: Lethal dose irradiation for BALB/c mice is typically 800-900 cGy and 1,000-1,200 cGy for C57B/6. The dose is typically split into two sessions of irradiation spaced at least 3-4 hours apart.
Continued from step 3.11, harvest transduced donor cells from the 6 well plates by gently pipetting supernatant into conical tubes. Wash each well with 1 ml of PBS to collect residual cells and add to 50 ml conical tubes.
Add 0.5 ml of 0.05% trypsin to wells and incubate at 37 °C in the tissue culture incubator for 5 min.
Add 1 ml D10 to wells and detach any remaining cells by gentle pipetting. Add cells to the respective tubes from step 4.2 and pellet by centrifugation at 4 °C for 10 min at 400 x g.
Wash cells with PBS and centrifuge at 4 °C for 10 min at 400 x g. Resuspend in 5 ml PBS and count cells using a hemocytometer by trypan blue exclusion. NOTE: If the vector has a GFP tag then quantify the percentage of GFP-positive cells with a flow cytometer.
Resuspend 5 x 10 - 2 x 10cells in 50 - 100 µl PBS for injection into mice.
Inject cells via retro-orbital injection into anesthetized mice using a sterile 27 G x ½" needle. NOTE: Other injection techniques include tail-vein, splenic, or femoral.
Anesthetize mouse using isoflurane and pinch foot to assess responsiveness.
Position the mouse on its side and restrain by using both the thumb and index finger such that the eye protrudes slightly from the head.
With the bevel facing up, insert the needle lateral to the medial canthus at a 45° angle. NOTE: If this technique is performed correctly, the eye should retract slightly and no resistance should be felt upon needle insertion.
Examine mouse for any signs of injury such as swelling or bleeding. NOTE: Following transplantation mice will have low blood counts for a number of weeks and so are susceptible to infection. Prophylaxis with antibiotics or use of acidified water may be used.
One month post-transplant, measure the % GFP in the peripheral blood as an indicator for engrafted donor cells by flow cytometry. NOTE: GFP alone cannot determine success of engraftment of the cells. The viral transduction may have failed yet engraftment may have occurred. In this case, no GFP cells would be detected, but engraftment of the transplanted cells was successful.
Take 10 µl of peripheral blood by puncturing the saphenous leg vein with a 21 G x 1 ½" syringe and add it to 100 mM EDTA in PBS to prevent coagulation.
Add 1 ml ACK to blood and lyse on ice for 10 min. Pellet cells by centrifugation at 400 x g for 10 min.
Aspirate supernatant in a vacuum flask and add 1 ml PBS supplemented with 2% FBS to stop lysis. Pellet cells by centrifugation at 400 x g for 10 min.
Aspirate supernatant in a vacuum flask and resuspend pellet in 100 µl PBS supplemented with 2% FBS.
Run samples on a flow cytometer and collect 300,000 events within the live cell gate (determined by FSC vs. SSC) and calculate the percentage of GFP and GFP cells.
Additionally at 1 month post-transplant, perform complete blood counts (CBC) using an automated veterinary hematology analyzerto monitor disease progression. NOTE: Continue to monitor disease by % GFP in peripheral blood and CBC monthly.
To terminate the experiment, anesthetize mouse using isoflurane and pinch foot to assess responsiveness. Sacrifice mouse by cervical dislocation and harvest spleen and bone marrow for histopathology. NOTE: The length of the experiment is subjective and the termination date should be assessed based on the disease phenotype expected.
1. Generation of Ecotropic Retrovirus
Prepare high-quality plasmids with a concentration of at least 1 µg/µl using either a commercial maxi-prep kit or cesium chloride purification. NOTE: These include an MSCV backbone vector encoding the gene of interest (in this case CALR) and marker of choice (GFP, Neo, etc.) as well as an ecotropic packaging plasmid, encoding gag-pol-env (referred here as plasmid).
Thaw and expand low-passage 293T cells in DMEM supplemented with 10% FBS and L-glutamine with penicillin/streptomycin (D10). Plate 5 x 10 cells in a 10 cm tissue culture-treated dish in a humidified tissue culture incubator at 37 °C and 5% CO2.
Expand 293T cells in culture. On the day before transfection, wash cells by adding 1 ml PBS and aspirate supernatant into a vacuum flask.
To trypsinize cells, add 2 ml 0.05% trypsin and incubate dishes in a humidified tissue culture incubator for 2 - 3 min at 37 °C and 5% CO2.
To stop trypsinization, add 3 ml D10 to dish and transfer cells to a 15 ml conical tube. Spin cells at 400 x g for 10 min.
Aspirate supernatant into a vacuum flask and resuspend cell pellet in 2 ml D10.
Count the cells by trypan blue exclusion using a hemocytometer.
Seed 2 x 10 cells per dish into three 10 cm tissue culture-treated dishes per virus generated. NOTE: For optimal results, do not allow the cells to exceed 30 - 50% confluence at time of transfection or a poor virus yield may be obtained.
Immediately before transfection, aspirate media into a vacuum flask and replace with 5 ml fresh D10.
For every 10 cm Petri dish to be transfected prepare an individual sterile 1.5 ml microcentrifuge tube.
Pipette 760 µl of reduced serum media into each microcentrifuge tube, then carefully add 40 µl of transfection reagent directly into the media. Incubate tubes in the tissue culture hood at room temperature for 5 min.
Add 30 µg of MSCV vector with gene of interest (15 µg if using empty vector) as well as 5 µg of plasmid to each respective tube and mix gently by pipetting up and down. Incubate at room temperature in the tissue culture hood for an additional 15 min. NOTE: Smaller vectors tend to have higher viral yields.
Carefully add the total volume of each reaction (approximately 800 µl) drop-wise into its respective 10 cm Petri dish and gently tilt the dish from side to side to mix. Return cells to the humidified tissue culture incubator.
Following an 8 hr or overnight incubation in tissue culture incubator, aspirate media into a vacuum flask and gently replace with 10 ml of fresh D10.
At 48 hr post-transfection collect supernatant into a 35 ml syringe and filter through a 0.45 µm membrane to remove cell debris.
OPTIONAL: Place 10 ml fresh D10 back on the 293T cells and additional virus may be harvested at 72 hr post-transfection.
Dispose of 293T cells in biohazard waste when no additional virus is collected.
Aliquot viral supernatant into single use volumes (for example 1 ml for virus titer or 6.5 ml for BM infection). Flash-freeze virus with liquid nitrogen and store virus at -80 °C. NOTE: Avoid repeated freeze/thaw cycles as they greatly reduce virus titer.
2. Determine Relative Viral Titer by Flow Cytometry
Thaw 3T3 cells and maintain in D10. Culture the cells in a 10 cm tissue-culture treated dish in a humidified tissue culture incubator at 37 °C and 5% CO2.
Perform viral titer in triplicate. To prepare cells, wash cells by adding 1 ml PBS and aspirate supernatant into a vacuum flask.
To trypsinize cells, add 2 ml 0.05% trypsin and incubate dishes in a humidified tissue culture incubator at 37 °C and 5% CO2.
To stop trypsinization, add 3 ml D10 to dish and transfer cells to a 15 ml conical tube. Spin cells at 400 x g for 10 min.
Aspirate supernatant into a vacuum flask and resuspend cell pellet in 2 ml D10.
Count the cells by trypan blue exclusion using a hemocytometer.
Seed 3T3 cells at a density of 1 x 10 cells into fifteen 60 mm tissue culture-treated dishes and incubate overnight.
Make 1:3, 1:10, 1:30, and 1:100 dilutions of thawed viral supernatant using D10 in a total of 1 ml. Also include a virus-free control.
Aspirate media from 3T3 cells into a vacuum flask and replace with 4 ml of D10.
Overlay the 3T3 cells with the dilutions of viral supernatant and add polybrene to a final concentration of 8 µg/ml to each dish. Incubate for 48 hr in the tissue culture incubator at 37 °C and 5% CO2.
Determine relative viral titer by flow cytometry:
To wash cells, aspirate the media into a vacuum flask and add 5 ml PBS.
Aspirate the PBS into a vacuum flask. Add 1 ml 0.05% trypsin and incubate at 37 °C for 2 - 5 min to detach cells from dish.
Add 3 ml D10 and pipette up and down to detach any remaining cells from the plate. Transfer the cells to a FACS tube and centrifuge at 400 x g for 10 min.
Decant supernatant and wash cells with 3 ml PBS. Centrifuge at 400 x g for 10 min and decant supernatant. Resuspend in 200 µl PBS.
Run cells on a flow cytometer. Collect between 20,000 - 30,000 events within the live cell gate (determined by FSC vs. SSC) and calculate the percentage of GFP and GFP cells. NOTE: The viral titer is considered acceptable when the 1:30 dilution of viral supernatant yields at least 50% GFP 3T3 cells. If this dilution results in less than 50% GFP cells then suboptimal transduction results may be obtained. The calculation to determine viral titer was adapted from Limon et al., Blood (1997).
To determine relative virus titer, use the equation: virus titer = particle forming units (PFU)/ml = [(Number of 3T3 Cells × Frequency of GFP Cells) / Volume of Supernatant (ml)] × Dilution Factor.
3. Transduce Donor Bone Marrow Cells
To prepare donor mice for bone marrow (BM) harvest, first anesthetize mice by isoflurane vaporizer with a flow rate of 5% combined supplemental oxygen at 1 L/min. Pinch foot to assess responsiveness. NOTE: Donor mice (less than 8 weeks old) should be prepared 5 days prior to bone marrow harvest (8 days prior to transplantation). One donor mice will provide enough cells for at least 2 recipients.
Inject 150 mg/kg 5-fluorouracil (5-FU) via retro-orbital injection in anesthetized mice using a 27 G × ½" needle. CAUTION! 5-FU an anti-cancer chemotherapeutic agent. Always handle 5-FU inside a certified chemical fume hood or a ducted biosafety cabinet. Consult with the institution's laboratory and animal safety committee to determine appropriate labeling of mice treated with 5-FU.
Position the anesthetized mouse on its side and restrain by using both the thumb and index finger such that the eye protrudes slightly from the head.
Starting with the needle lateral to the medial canthus and with the bevel facing up, insert the needle at a 45° angle in the medial direction and stop when the needle is halfway inserted. Slowly inject cells and remove carefully remove needle. NOTE: If this technique is performed correctly, the eye should retract slightly and no resistance should be felt upon needle insertion.
Examine mouse for any signs of injury such as swelling or bleeding.
Harvest bone marrow 5 days after 5-FU treatment (3 days prior to transplantation).
Anesthetize mice by isoflurane vaporizer with a flow rate of 5% combined supplemental oxygen at 1 L/min. Pinch foot to assess responsiveness.
Sacrifice mouse by cervical dislocation. Sterilize mouse by spraying generously with 70% EtOH until fur becomes wet.
Using dissecting scissors, make an incision in the skin and dissect the fascia away from the leg muscles. Next, dissect the leg away from mouse by severing the femur at the hip and the tibia at the ankle.
Bend the leg into a "L" shape and separate each leg bone by cutting at the knee joint with dissecting scissors.
To remove cartilage at the distal ends of each leg bone, use the dissecting scissors to gently scrape muscle towards one end of the leg bone until cartilage is disengaged.
Using a syringe with a 27 G x ½ inch needle, flush each leg bone with PBS supplemented with 2% FBS over a 100 µM nylon membrane in a 50 ml conical tube. Flush bone until bone turns white to maximize the number of cells harvested.
Use the plunger of a syringe to mash cells through the nylon membrane into the 50 ml conical tube to obtain a single cell suspension. Repeat with other mouse leg.
Centrifuge cells at 4 °C for 10 min at 400 x g and discard supernatant. Resuspend BM in 5 ml ammonium chloride potassium (ACK) buffer to lyse red blood cells. Incubate cells on ice for 10 min.
Fill tube with PBS to stop cell lysis. Centrifuge cells at 4 °C for 10 min at 400 x g and discard supernatant. Repeat lysis step if the BM pellet has red color.
Resuspend in 5 ml PBS and count cells by trypan blue exclusion using a hemocytometer.
Resuspend cells at 2 x 10 cells per m with 2x pre-stim cocktail which contains DMEM supplemented with 20% FBS, L-glutamine, penicillin/streptomycin, IL-3 (14 ng/ml), IL-6 (24 ng/ml), and SCF (112 ng/ml). Plate 2 ml per well in 6 well plates.
Incubate the cells overnight at 37 °C and 5% CO2.
Add 2 ml of viral supernatant to each well containing BM cells and add polybrene (8 µg/ml). Spin plates at 30 °C for 90 min at 1,500 x g then return plate to the tissue culture incubator overnight.
Pipette cell suspension into conical tubes and centrifuge at 4 °C for 10 min at 400 x g, do not discard the plate. Resuspend cells in 2 ml fresh 2x pre-stim cocktail per well and return to the original wells.
Perform a 2 spinoculation by repeating steps 3.7-3.9.
4. Transplant Donor Cells into Recipient Mice
Prepare syngeneic recipient mice for transplant with lethal dose total body irradiation < 24 hr prior to injection of BM cells. NOTE: Lethal dose irradiation for BALB/c mice is typically 800-900 cGy and 1,000-1,200 cGy for C57B/6. The dose is typically split into two sessions of irradiation spaced at least 3-4 hours apart.
Continued from step 3.11, harvest transduced donor cells from the 6 well plates by gently pipetting supernatant into conical tubes. Wash each well with 1 ml of PBS to collect residual cells and add to 50 ml conical tubes.
Add 0.5 ml of 0.05% trypsin to wells and incubate at 37 °C in the tissue culture incubator for 5 min.
Add 1 ml D10 to wells and detach any remaining cells by gentle pipetting. Add cells to the respective tubes from step 4.2 and pellet by centrifugation at 4 °C for 10 min at 400 x g.
Wash cells with PBS and centrifuge at 4 °C for 10 min at 400 x g. Resuspend in 5 ml PBS and count cells using a hemocytometer by trypan blue exclusion. NOTE: If the vector has a GFP tag then quantify the percentage of GFP-positive cells with a flow cytometer.
Resuspend 5 x 10 - 2 x 10cells in 50 - 100 µl PBS for injection into mice.
Inject cells via retro-orbital injection into anesthetized mice using a sterile 27 G x ½" needle. NOTE: Other injection techniques include tail-vein, splenic, or femoral.
Anesthetize mouse using isoflurane and pinch foot to assess responsiveness.
Position the mouse on its side and restrain by using both the thumb and index finger such that the eye protrudes slightly from the head.
With the bevel facing up, insert the needle lateral to the medial canthus at a 45° angle. NOTE: If this technique is performed correctly, the eye should retract slightly and no resistance should be felt upon needle insertion.
Examine mouse for any signs of injury such as swelling or bleeding. NOTE: Following transplantation mice will have low blood counts for a number of weeks and so are susceptible to infection. Prophylaxis with antibiotics or use of acidified water may be used.
One month post-transplant, measure the % GFP in the peripheral blood as an indicator for engrafted donor cells by flow cytometry. NOTE: GFP alone cannot determine success of engraftment of the cells. The viral transduction may have failed yet engraftment may have occurred. In this case, no GFP cells would be detected, but engraftment of the transplanted cells was successful.
Take 10 µl of peripheral blood by puncturing the saphenous leg vein with a 21 G x 1 ½" syringe and add it to 100 mM EDTA in PBS to prevent coagulation.
Add 1 ml ACK to blood and lyse on ice for 10 min. Pellet cells by centrifugation at 400 x g for 10 min.
Aspirate supernatant in a vacuum flask and add 1 ml PBS supplemented with 2% FBS to stop lysis. Pellet cells by centrifugation at 400 x g for 10 min.
Aspirate supernatant in a vacuum flask and resuspend pellet in 100 µl PBS supplemented with 2% FBS.
Run samples on a flow cytometer and collect 300,000 events within the live cell gate (determined by FSC vs. SSC) and calculate the percentage of GFP and GFP cells.
Additionally at 1 month post-transplant, perform complete blood counts (CBC) using an automated veterinary hematology analyzerto monitor disease progression. NOTE: Continue to monitor disease by % GFP in peripheral blood and CBC monthly.
To terminate the experiment, anesthetize mouse using isoflurane and pinch foot to assess responsiveness. Sacrifice mouse by cervical dislocation and harvest spleen and bone marrow for histopathology. NOTE: The length of the experiment is subjective and the termination date should be assessed based on the disease phenotype expected.
Representative Results
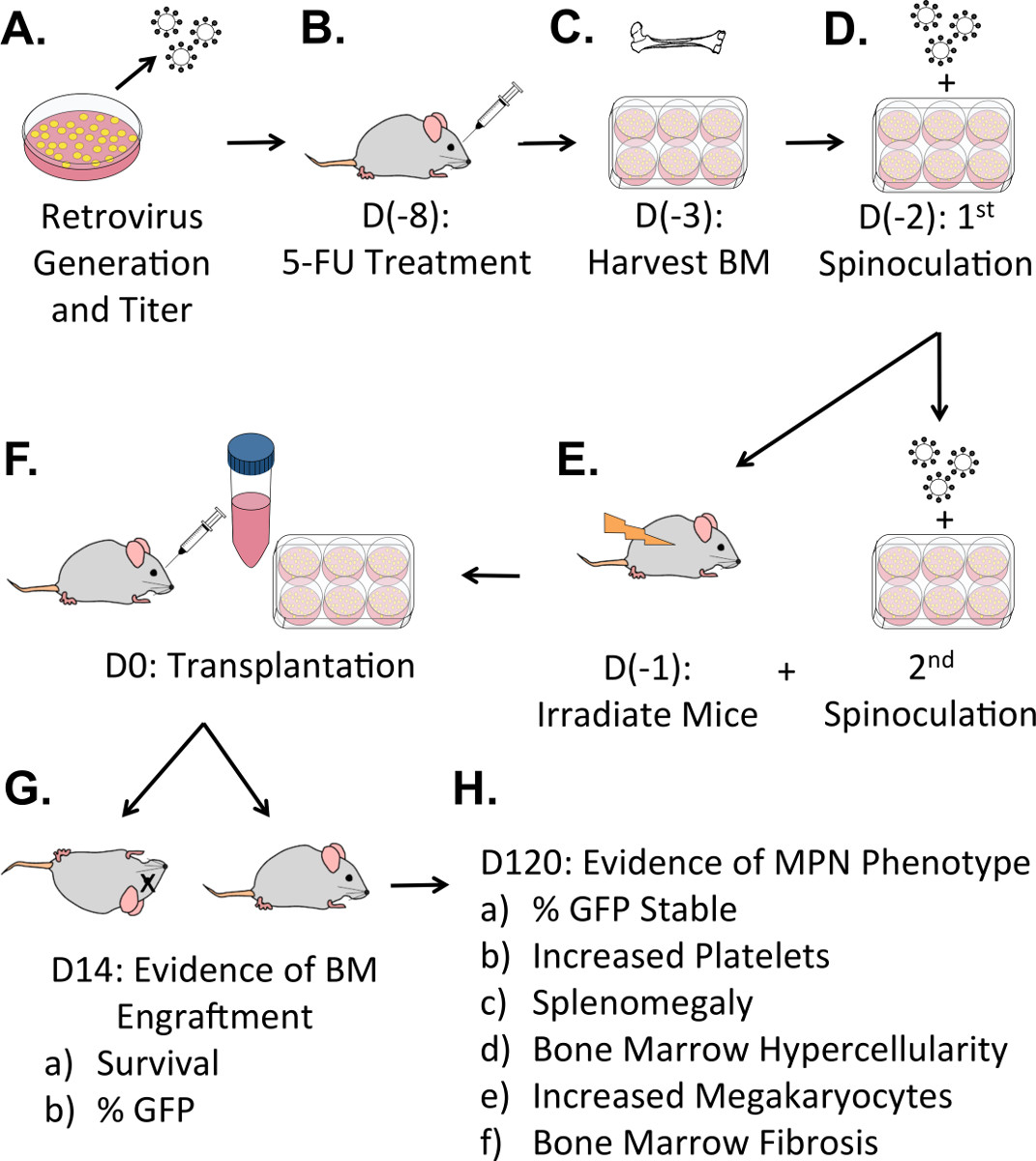
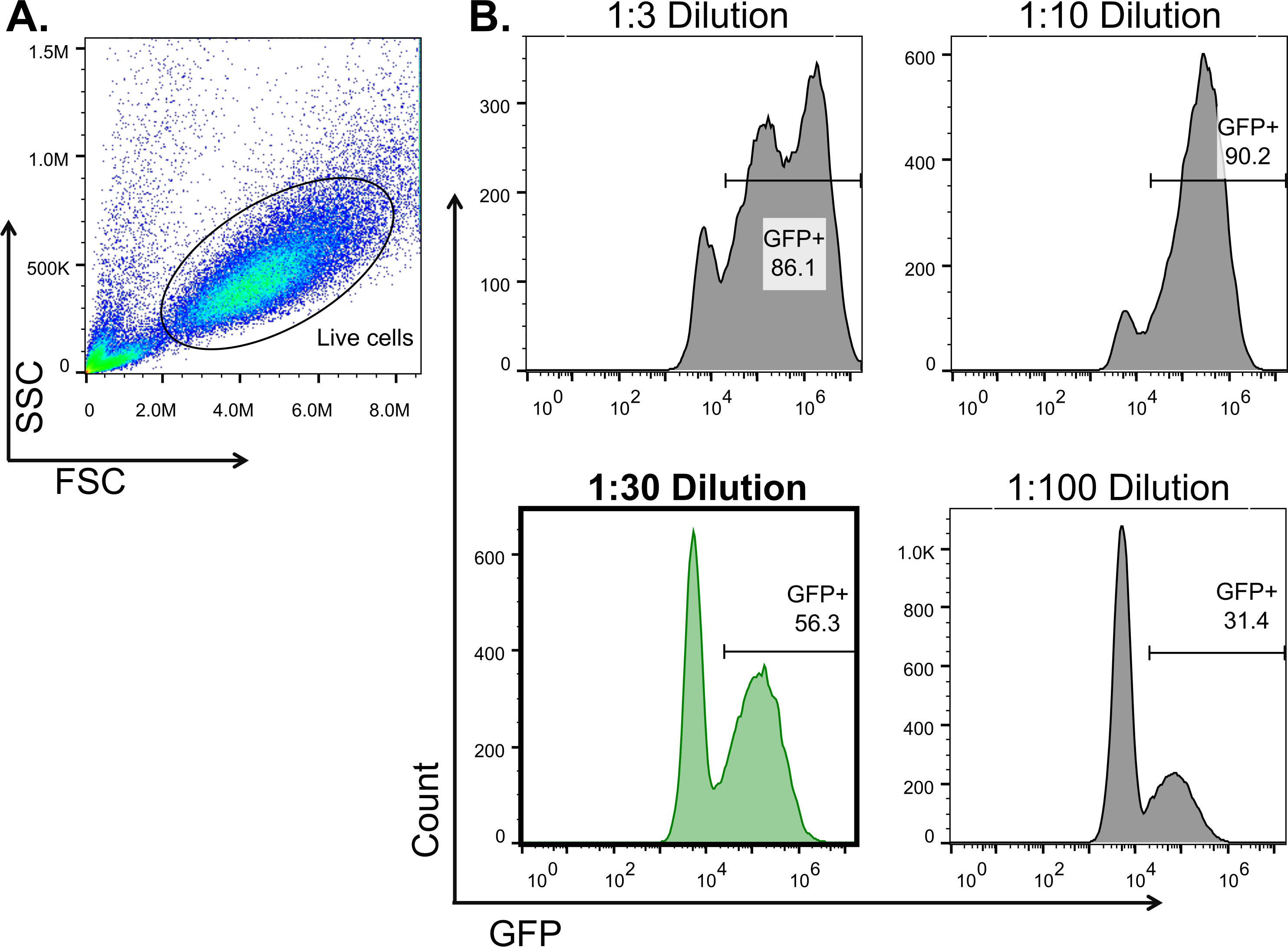
The transduction-transplantation technique results in hematopoietic reconstitution of the recipient mice with cells expressing the gene of interest. Figure 1 shows an overview of the transduction-transplantation mouse model of calreticulin mutated MPN. Briefly, retrovirus expressing CALRwt or CALRdel52 is used to infect BM cells from a C57B/6 donor mouse. Transduced cells are transplanted into irradiated C57B/6 recipient mouse and donor cell engraftment occurs during the first month post-transplant. Evidence of a disease phenotype becomes apparent 3 months post-transplant where mice exhibit increased platelets and megakaryocytes, followed by bone marrow fibrosis at 6 - 10 months post-transplant. If donor cells fail to engraft, mouse death may occur within the first 2 weeks following transplant. In addition to poor injection or trauma during injection, other technical errors can cause poor engraftment of transduced cells or mouse death. These include sub-optimal irradiation of recipient mice, if this occurs most hematopoietic cells will be of recipient rather than donor origin. On the other hand, excessive irradiation of recipients can cause mice to develop irradiation-induced sickness or even death. Low viral titers will result in low infection efficiency of donor cells. As a consequence low numbers of donor cells will express the gene of interest and so mice may not demonstrate the desired phenotype. For this reason, it is crucial that virus with high titers is used to transduce donor cells. Figure 2 illustrates how to calculate relative viral titer where the % GFP is calculated from events collected from the live cell gate. Figure 2B illustrates a titer with more than one viral particle per cell (1:3 dilution) as well as titers with single viral particles per cell (1:30, 1:10, and 1:100 supernatant). Ideally, at least 50% GFP cells would be detected with 1:30 dilution of viral supernatant. Figure 3 shows evidence of a successful transplant recipient where CALRdel52 mice exhibit an MPN phenotype with increased platelets, increased megakaryocytes in the bone marrow, and bone marrow fibrosis.

Figure 1: Overview of Transduction-Transplantation Mouse Model of Myeloproliferative Neoplasms.A) Retrovirus generation and determination of viral titer occurs 1 - 2 weeks prior to transplant. B) D(-8) (five days prior to bone marrow harvest), donor mice are treated with 5-FU to deplete lineage committed cells and induce hematopoietic stem cell cycling. C) On D(-3), bone marrow is harvested from leg bones and cultured in 2x pre-stim overnight to induce cell cycling of hematopoietic stem cells. D) Donor cells are infected with viral supernatant on D(-2) and the cells are centrifuged at 400 x g at 30 °C for 1.5 hr for the 1 spinoculation. E) On D(-1), a 2 spinoculation is performed on donor cells. Additionally, mice are irradiated to deplete cells in the host bone marrow niche to allow for donor cell engraftment. F) Transduced donor cells are transplanted into irradiated syngeneic recipient mice on D0. G) If donor cells fail to engraft then death will occur by day 12 - 14 following transplant if lethal dose irradiation has been used. H) The MPN phenotype becomes evident by 3 months post-transplant. Please click here to view a larger version of this figure.
{kind=link}

Figure 2: Determination of Viral Titer by Flow Cytometry. 3T3 cells are transduced with different concentrations of virus and transduction efficiency is monitored via flow cytometry. A) Events are collected within the live cell gate as visualized by FSC vs. SSC. Dead cells are excluded from GFP analysis. B) Histograms show % GFP for each volume of viral supernatant tested. The viral titer is acceptable when at least 50% of 3T3 cells are GFP when infected with the 1:30 dilution of viral supernatant. Using the equation from step 2.11.6, the viral titer was calculated based on a cell count of 400,000 cells. The calculation for viral titer at a 1:30 dilution follows: [(400,000 x 0.56)/1) x 30] = 6.72 x 10 PFU/ml. Per step 3.7, infecting 4 x 10 cells with 2 ml of viral supernatant would result in each cell receiving 3 viral particles. Please click here to view a larger version of this figure.
{kind=link}

Figure 3:Evidence of Successful Donor Cell Engraftment and MPN Phenotype. Irradiated recipient mice surviving beyond 2 weeks post-transplant indicates successful engraftment of injected cells. A) Transplanted donor cells can be monitored by % GFP in peripheral blood. B) Additionally, CBC counts should be taken to monitor disease progression. Increased platelets are detected as early as 2 months post-transplant in CALRdel52 when compared to CALRwt and empty vector control. C) At the time of termination, CALRdel52 mice exhibit classic features of the MPN phenotype including splenomegaly (not shown), bone marrow hypercellularity, expansion of megakaryocytes in the bone marrow, and bone marrow fibrosis. Please click here to view a larger version of this figure.
{kind=link}
| Technical Error | Causes | Result |
| Poor Injection or Trauma | Transplant Rejection | Transplant Failure |
| Bad Quality of Donor Cells | Transplant Rejection | Transplant Failure or Death |
| Low Virus Titer | Poor Transduction of HSC | Transplant Failure |
| High Irradiation Dose | Irradiation induced sickness | Death |
| Low Irradiation Dose | Transplant Rejection | Transplant Failure |
| Old Donor Mice (+12 Weeks) | Low HSC Input | Transplant Failure |
Table 1: Technical Errors that can Result in Mouse Death or Transplant Failure. This table lists examples of technical errors and their associated causes that could occur with bone marrow transplant protocol.
Discussion
This protocol provides a detailed description of how to perform bone marrow transplants in mice to recapitulate an essential thrombocythemia-like disease with progression to myelofibrosis with CALRdel52 mutation as the driver of disease. Successful transplantation of cells expressing CALRdel52 results in increased platelets, expansion of megakaryocytes, and bone marrow fibrosis. As bone marrow transplantation is a multistep process, it is important to acknowledge steps where technical error can be avoided to prevent poor engraftment of cells expressing the gene of interest or even mouse death.
A critical factor to a successful transduction-transplantation model that is often overlooked is the quality of virus. Virus with high titers facilitates good transduction efficiency and thus a strong basis for disease, whereas using a virus associated with low titer will result in fewer cells expressing the gene of interest. Transduction efficiency can be enhanced by reagents that increase contact between virus and cells such as polybrene and retronectin. Transduction of HSCs is known to be difficult even with high concentrations of virus, ecotropic retrovirus only infects dividing cells. The purpose of "pre-stim" media (containing SCF, IL-3, and IL-6) is to induce cycling of quiescent HSCs. The lentiviral system could be used as an alternative approach if infection of non-dividing cells is necessary.
Another factor that can have an effect on virus generation is the type of transfection reagent used. Optimal transfection reagents should be determined empirically as marked differences in cell toxicity have been observed between research groups. The transfection reagent used here has resulted in good viral yield with low cell toxicity. Other common transfection reagents include calcium phosphate and nonliposomal transfection reagent such as Fugene. This protocol uses plasmid as the packaging vector with specific tissue trophisms for mouse and rat. If considering other animal models for transduction-transplantation, other packaging vectors with broader trophisms could also be used to generate amphotrophic (mouse, rat, human) or pantrophic (broad range trophisms) retrovirus.
An added advantage to the bone marrow transduction-transplantation model is the ability investigate the competitive advantage of two different donor populations or to express multiple genes of interest simultaneously by using unique markers to designate each population of interest. Such transplants often utilize congenic C57BL/6 mice to track donor cells beyond the use of an integrated GFP marker. Because congenic C57BL/6 mice can express leukocyte markers for either CD45.1 or CD45.2, donor cells can be obtained from one background and transplanted into the other. Moreover, a hybrid F1 strain can be generated to produce offspring expressing both CD45.1 and CD45.2 markers. Alternatively, the MSCV retroviral vector is available with several different tags, including unicistronic (e.g., FLAG HA) or bicistronic (e.g., GFP, RFP, YFP, mCherry, hCD4) constructs. These constructs may be used concurrently in competitive transplants to enable discrimination among donor populations and can be especially useful in situations where differentiation via CD45.1/CD45.2 expression is not available, such as the BALB/c mouse strain.
Another advantage of transduction-transplantation is the ability to investigate the contributions of specific cell types to disease initiation. While this protocol describes only the transduction-transplantation of whole bone marrow, other experimental designs may necessitate the enrichment or isolation of different HSC compartments. In these cases, the number of donor cells will vary according to the specific donor population used. Additionally, rescue cells from a naïve donor should be used as a supplement to support the mouse until HSC engraftment and expansion can occur. Table 2 outlines the recommended number of donor cells for transplantation of the various bone marrow compartments-.
| # of Cells / Transplant Recipient | # of Support Cells / Transplant Recipient | |
| Whole Bone Marrow | 500,000-2,000,000 | n/a |
| c-Kit+ | 1,000-10,000 | 200,000 |
| Lin-c-KitSca-1 (LKS) | 100-10,000 | 200,000 |
| LKS CD150CD48 SP | 1-100 | 200,000 |
| LKS CD150CD34- | 1-100 | 200,000 |
Table 2. Number of Donor Cells to Transplant.
Furthermore, secondary transplant may also be performed to assess the ability of transduced cells to serially transplant disease.
Transduction-transplantation is a highly versatile method that is much faster and significantly more cost efficient as compared to transgenic, knock-in, or xenograft models. It allows one to quickly determine whether the gene of interest is sufficient to induce a hematologic malignancy, and can be used as an in vivo pre-clinical model to test drugs. Other benefits of the transduction-transplantation technique are that it avoids expression in non-hematopoietic cells and that the retroviral insertion site serves as a clonal marker. Limitations of this technique include non-physiological levels of transduced gene and differences in the integration site of the gene. Taking all of the above mentioned benefits and limitations into account, transduction-transplantation is the obvious choice for initial in vivo modeling of putative hematopoietic oncogenes.
Disclosures
The authors have nothing to disclose.
Abstract
Transduction-transplantation is a quick and efficient way to model human hematologic malignancies in mice. This technique results in expression of the gene of interest in hematopoietic cells and can be used to study the gene's role in normal and/or malignant hematopoiesis. This protocol provides a detailed description on how to perform transduction-transplantation using calreticulin (CALR) mutations recently identified in myeloproliferative neoplasm (MPN) as an example. In this protocol whole bone marrow cells from 5-flurouracil (5-FU) treated donor mice are transduced with a retrovirus encoding mutant CALR and transplanted into lethally irradiated syngeneic hosts. Donor cells expressing mutant CALR are marked with green fluorescent protein (GFP). Transplanted mice develop an MPN phenotype including elevated platelets in the peripheral blood, expansion of megakaryocytes in the bone marrow, and bone marrow fibrosis. We provide a step-by-step account of how to generate retrovirus, calculate viral titer, transduce whole bone marrow cells, and transplant into irradiated recipient mice.
Acknowledgments
This work is supported by the V Foundation Scholar (AGF) and the MPN Research Foundation (AGF).